Dr. Vishal Singh*
Dr. M.L. Jain**
Ms. Archana Saxena***
Abstract
Availability of quality health care services, adopting safe health care practices, and health-seeking behavior by the community are the keys for preventing significant maternal, neonatal, and child deaths and bringing improvement in the health status of women and children. Rajasthan has trailed in many healthcare indicators, such as maternal mortality ratio (244, SRS 2014) infant mortality rate (46, SRS 2014 live births in 2013, SRS), footnote SRS-14. To bring improvement in the scenario, an integrated, evidence-based communication strategy, using the life cycle and continuum of care approach is critical in addressing the barriers and enabling the adoption of key behaviors and practices at home, community, and facility (healthcare centers/ hospitals) levels.
To provide a strategic action plan to the state based on SBCC strategy for RMNCH+A for increasing demand, use, and adoption of positive practices by families and communities, enhance the capacity of the existing manpower and develop a plan-of-action for narrowing the gaps in service provision and service utilization by a targeted beneficiary, a project titled ‘Strengthening Social and Behaviour Change Communication (SBCC)’ was implemented by SIHFW with support from UNICEF. The interventions focused on 10 High Priority Districts of Rajasthan.
Various innovative interventions such as the development of SBCC strategy on RMNCH+A and RI, collective training of ANM, ASHA, and Anganwari Workers (3As), the involvement of traditional and faith-based healers/ influencers, use of IPC tool contributed to the process of behavior change based on identified barriers. Process documentation of the innovations is presented in this research paper.
Background
There is increased recognition that availability of quality healthcare services, adopting safe health care practices and health-seeking behavior by the community are keys for preventing significant maternal, neonatal, and child deaths and bringing improvement in the health status of women and children.
Over the years the health care delivery system of Rajasthan got strengthened in terms of the availability of infrastructure which has created easy access to healthcare facilities down to the village level. The efforts are visible in the data related to maternal mortality, infant mortality, exclusive breast-feeding, and immunization, but the progress has been relatively slow. Rajasthan has trailed in many healthcare indicators such as maternal mortality ratio (244, SRS 2014) infant mortality rate (46, SRS 2014 live births in 2013, SRS), footnote SRS-14. Even the exclusive breastfeeding practices and full immunization figures are not very encouraging. Only 65.5% of women exclusively breastfeed their children between 0-5 months of age (DLHS-3) and 74.2% of the children are fully immunized (AHS12-13).
The continuum for maternal, newborn, and child health usually refers to the continuity of individual care and is critical throughout the lifecycle (adolescence, pregnancy, childbirth, the postnatal period, and childhood) and also between places of caregiving (including households and communities, outpatient and outreach services, and clinical-care settings).
However, an integrated, evidence-based communication strategy, using the life cycle and continuum of care approach is critical in addressing the barriers and enabling the adoption of key behaviors and practices at the home, community, and facility (healthcare centers/ hospitals) levels. Under the continuum of care, there are two dimensions-Stages of the Life cycle and places where the care is provided (these together constitute the ‘Continuum of Care’).
Life cycle (stages) herein includes Reproductive Stage, Maternal Stage, Neonatal Stage, Child Stage, and Adolescent Stage. The places where service or care is provided are the Service Delivery Platforms including-Home Based Care, Community Out-reach Care, and Facility (Hospital) Based Care. This whole strategic approach towards the stages is coined as RMNCH+A strategy. The ‘Plus’ (+) in the strategic approach denotes the inclusion of adolescence as a distinct ‘life-stage’ in the overall strategy. 16 indicators have been identified for monitoring the progress and improvement of interventions continuously.
In Rajasthan, the focus of priority actions is along the continuum of care for the mother from pregnancy to postnatal care up to 12 months after birth (pre-pregnancy and one-year-old infant) stages of the life cycle of the mother and child. The three Frontline workers and service providers of the two flagship programs NRHM and ICDS – ANM, ASHA, and AWW (Auxiliary Nurse Midwife, Accredited Social Health Activist, and Anganwari Workers) – address the needs of the beneficiary groups of mothers and children. A Rapid Assessment of MCH Services in five high focus districts in Rajasthan conducted by UNICEF (2010-2011) and Bottleneck Analysis revealed that there are gaps in knowledge, skills, capacity, and coordination in the functioning of 3As. The district analyses revealed that there are gaps in commodities, supply, and demand, and quality issues with regards to services. While the supply side issues cover Information Education Communication/ Behavior Change Communication (IEC/BCC) materials and Job Aids, tool gaps under Communicationthe demand-side look at issues of inadequate counseling and reach or exposure of messages by Frontline workers (3As).In the continuum of care points of contact of a family with FLW at homes, facility, or outreach there are windows of opportunity for integrated counseling that is being missed.
SIHFW (partnering with the Department of Medical and Health and UNICEF) undertook a KABP study of families and communities in five districts (2009) which introduced the State BCC strategy for NRHM in 2010. The findings of the study revealed many gaps of knowledge and behavior patterns of the community. Some of the recommendations the study made included -the need for enhancement of skills of 3As for IPC, addressing the communication gaps piloting the BCC and Trial for Improved Practices through counseling and observation and counseling skills of the service provider at health facilities should also be enhanced hand in hand. The study also recommended addressing these gaps through a comprehensive BCC Strategy covering all elements of behavior change communication interventions, region-specific BCC plans, socio-culturally suitable approaches focused on IPC, reinforcement through mass-media, mid-media/large scale community-based activities, and innovations.
Over time, a need has emerged to update the existing BCC Strategy for Health under NRHM, in the context of the integrated approach of RMNCH+A delivery of services with a focus on the 1000-day window of opportunity for mother and child. The studies and analyses made it evident that effective Inter-Personal Communication (IPC) is required for counseling the target audience for desired behavior. From the above-mentioned researches and many others, it was realized that a comprehensive approach towards Behavior Change Communication will further help in the achievement of current targets of reducing the Infant Mortality Rate, Maternal Mortality Ratio, Total Fertility Rate, and quality of service delivery up to the unreached population.
Hence, a project was implemented by SIHFW, which lead to an overall strengthening of existing services for the community and implementing innovative actions covering the RMNCH+A in the state.
About the Project
The project ‘Strengthening Social and Behavior Change Communication (SBCC)’ is implemented by SIHFW with support from UNICEF. The interventions focused on 10 High Priority Districts of Rajasthan (Bundi, Badmer, Banswara, Dholpur, Dungarpur, Jalore, Jaisalmer, Karauli, Rajasamand, and Udaipur).
Objectives of the project
- To provide a strategic action plan to the state based on SBCC Strategy for RMNCH+A for increasing demand, use, and adoption of positive practices by families and communities.
- To enhance the capacity of the existing manpower with enhancement supportive BCC tools/kits, in addition to training and supportive supervision for frontline workers.
- To scan and develop a plan-of-action for narrowing the gaps in service provision and service utilization by targeted stakeholders.
Key Interventions
Technical Working Group (TWG) for SBCC and Consultation Platforms
For purpose of reviewing the progress and consultations for planning and challenges, a Technical Working Group (TWG) was constituted. Its purpose was to obtain the guidance and support to strengthen SBCC in the state and to focus on conceptualizing, planning, implementation, and monitoring of health communication at the state, district, and block levels. The group included officials from DMHS, IEC Bureau, experts from PSI, UNICEF, UNFPA, Save the Children, IHBP, etc. Meetings at regular intervals were organized at SIHFW.
Strategy Documents on SBCC for RMNCH+A and Routine Immunization
The strategy documents were developed by adopting “bottom to top” methodology, Orientation cum consultation workshops were organized, and Zonal District Block and community level officials were involved- CMHO, RCHO, Divisional Coordinators, District IEC Coordinator, District ASHA Coordinator, and Focused District Coordinator of development partners, In the planning process Socio-Cultural Determinants of Community and behaviors in the continuum of care in Rajasthan considered. This has helped in obtaining the ‘voice from the fields’ (experiences of frontline workers, which were considered to form the basis for a strategy for the first time ever).
The barriers related to behavior and services
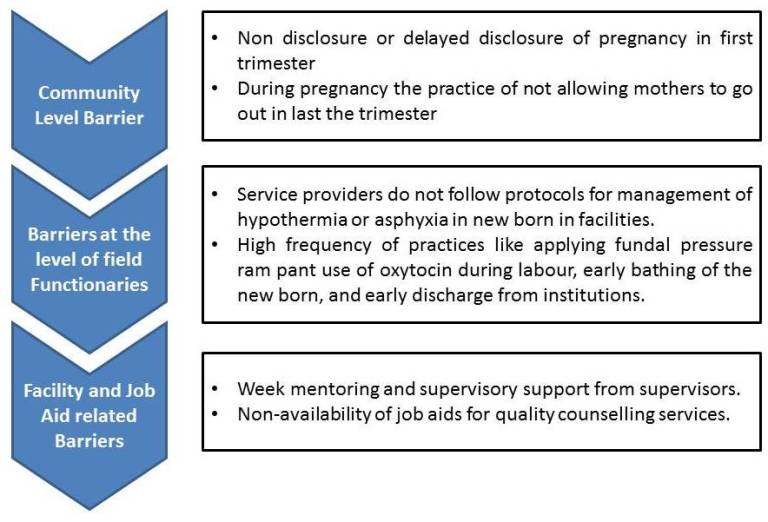
For the above-identified barriers, the following areas were suggested by the HPD district teams for action in their respective plans:
- Capacity building of 3 As
- Innovations and use of local media (Promotion of TIPS/PDA during a Home visit by ASHA)
- E-ASHA
- Community interaction /meeting-VHSC, VCD
- Saas -Bahu (Mother-In Laws-Daughter In-Laws meeting together)
- Supervisory visits for handholding support by IEC Team
- Use of Job Aids.
As an outcome, Strategy Documents on Social and Behavior Change Communication for RMNCH+A (and Routine Immunization were developed by SIHFW and were shared with NRHM, and States
Capacity Building Interventions
Because of the strategy documents and recommended skill enhancement of field functionaries by many above-cited research reports recommended, a plan was developed to address the above gaps through focused capacity building of 3As to make them capable enough to work in the form of village-level Communication Resource Teams.
There were a series of consultations for finalizing the communication capacity interventions. The outcomes of all the consultations leading to the finalization of thematic areas and the IPC tool kit. Primarily Tool kit used by PSI was adopted. Capacity Building Plan was finalized with the following Communication Objectives:
- To develop skills of 3As to find out the areas of healthcare services which are lacking in utilization by the community such as ANC, PNC, New Born Care, Immunization and Family Planning.
- To develop skills of 3As to identify the barriers in terms of reasons for low utilization, through discussion methods including IPC (Counseling), Home visits, FGDs, and village meetings.
- To strengthen village-level community processes including MCHN day and VHSNC through modification in guidelines and orientation of 3As for implementation.
Training of Trainers (ToTs)
To develop manpower resource for capacity building and handholding of other interventions of SBCC, training of trainers were organized at SIHFW.
Trainers were trained on SBCC and interpersonal skills, social mapping, key steps of behavior change, social inclusion and exclusion, etc. An integrated approach was adopted for training the trainers wherein training contents and materials of PSI, IHBP, NRHM-Save the children, and NCIS were integrated and used.
Seventy trainers were trained in three batches of ToT wherein a mix of District IEC Coordinators, District ASHA coordinators and PHNs, BPMs, LHVs, etc were trained as trainers in SBCC and IPC. There was an average increase of 10 points in every batch of ToT, which indicates learning in terms of knowledge and skill development.
Training of 3As

As a pilot activity, 3As –ANM, ASHA, and Anganwari Workers of the four HPDs of Unicef-Dungarpur, Banswara, Jalore, and Barmer were trained at one block in each HPD in a two days training. The blocks were: Baytu in Barmer, Ahore in Jalore, Bichiwara in Dungarpur, and Partapur in Banswara.
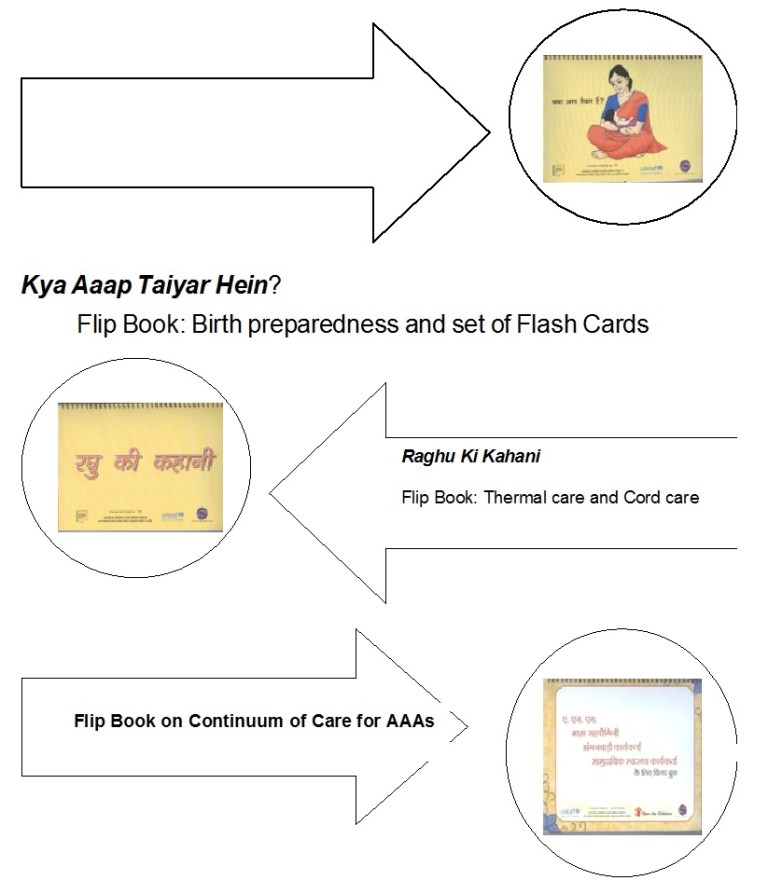
The training was organized with an objective of orientation and skill development of 3As on Interpersonal Communication skills. The 3As were trained on key factors of AAAs with mock IPC sessions to emphasize learning by doing. A set of IPC tool kits were also provided to the trained participants. The kit included Flipbooks and Birth Preparedness (KyaAapTaiyaar Hein), Thermal and Cord Care (Raghu kiKahani) and Continuum of Care for Field Functionaries, and a set of Flash Cards with Birth preparedness.
“During training with the frontline workers, I constantly attempt to motivate them and make the training more participative and interactive”.
– DAC, Karauli
The training was imparted by SBCC/ IPC District Trainers already trained at SIHFW in ToT organized under SBCC partnership with UNICEF. The training program was implemented in pilot blocks of the 4 HPDs-Barmer (Baitu), Jalore (Ahore), Banswara (Partapur), and Dungarpur (Bichiwada). All the batches of this training were monitored by the SIHFW team, with immediate payments of honorarium and accounts clearing after training completion of each batch.
Communication Model: Capacity Building and Behavior Change
For an academic and conceptual understanding of the partnership, the following Communication model was adopted by AAAs to use Inter-Personal Communication (IPC) and review the feedback as shown in the figure below:
“When you see something, you remember it. When you do something, you learn it”
– DRIC, Bikaner

Sector Meeting Level Training -3As
After analyzing the piloting results and consultations, there were modifications done in the implementation plan and approach of capacity building of 3As. In total, about 83 sessions were organized at Sector Meetings. Some sessions, district wise is Dholpur-10, Barmer-10, Jalore-2, Jaisalmer-8, Banswara-10, Dungarpur-10, Bundi-9, Rajasamand-6, Udaipur-10, and Karauli-8.
This is an innovative activity and is being carried out for the first time in the state since the orientation focuses on the combined improvement of communication skills of field functionaries and for the first time a capacity-building activity was organized at sector meetings, thereby strengthening the mechanism of sector meetings.
Faith-Based Healers an agent of Change
Based on research, it was found that many families and individuals still have more faith in the traditional healer rather than the modern system of medicine to cure public health problems. A pool of opinion makers/religious leaders/ BHOPAs was selected with the exhaustive exercise of selection by the involvement of community-level health functionaries. They and the HPDs, about 175 in all, were oriented to mobilize the community for accepting the RMNCH+A services. Faith-based healers were identified to mobilize the outreach population and ensure service utilization by the community. It was planned that faith-based healers will play the role of the catalyst and change maker. As a result, some changes have been noted in the immunization program in certain blocks.
IPC Tool Kits with 3As for Counseling
The IPC tool kits (including 3 Flip Books and 1 set of Flash Cards) were adopted after consultation with partner agencies such as PSI and IEC Bureau. Research has shown that pictures are effective in health education. Findings of many studies indicate that pictures closely linked to written or spoken text can be effective to conceive the message, when compared to text alone, by markedly increasing attention to and recall of health education information. Pictures can also improve comprehension when they show relationships among ideas or when they show spatial relationships. Patients with very low literacy skills can be helped by spoken directions plus pictures to take home as reminders or by pictures plus very simply worded captions (source: Patient Education and Counseling, Vol 61, Issue 2, May 2006)
The tool kit is being widely used by trained AAAs. This has been observed through monitoring of MCHN(Maternal and Child Health Days) and field assessment in 4 HPDs. Trained manpower is showing confidence in using the tool kits as support to counseling and awareness among the community.
Amma Ji Kehti Hein- A set of DVD kit containing short films on the following 11 themes was sent to each block of all 10 HPDs. Also, all the Districts HQs of Rajasthan were provided the films are on themes- Teekakaran Kaise Bachata Hai, Teekakaran -Garbhavasthaaur Tetanus, Teekakaran-Pehlevarsh me Sabhiteeke, Teekakaran-Teeke Kahan Uplabdh Hein, Surakshit Matrutva-ANC check-up, Surakshit Matrutva-Institutional Delivery, Surakshit Matrutva-Aahar, and Aaaram, Surakshit Matrutva-Danger Signs, Care of the New Born, Teen Deriyan and JeevanBharkiSuraksha.
Films in Tarang DVD Kit-The Tarang module developed by UNICEF (Country Office)contains six films on- BadhteKadam, Ek Din ZindagiKa, EkNayiSubah, RachnatmakRavaiya, How to Use Communication Materials and I am Dalit –How are You. These films are based on good and bad practices of community dialogue, counseling (Inter-Personal Communication) done by Field Level Functionaries (AAAs). The films have pause buttons to take feedback from the audience during the film shows, for understanding and reiteration of messages. Films on health awareness and IPC skills were adopted from UNICEF (Ammaji and Tarang DVDs). Same as IPC Tool kits, the films were adopted as it is and not re-developed. The films of the AmaJi series were copied into DVDs and distributed to Blocks while the DVD of the Tarang training kit was provided to trainers. Some studies also found films to be an effective medium in making learning easier to understand and for message recall. For example, The film show was found effective in increasing the knowledge score of school children by three-fold from pre-test (The Nursing Journal of India, Nov 2011).
DVD films were shown at capacity building interventions on SBCC/IPC at all levels-State, District, Block, and Sector. The DVD kits will continue to be utilized, even after the SBCC partnership between SIHFW and UNICEF is closed, for community-level IPC sessions. Also on MCHN days, films are being used for film shows for creating awareness among the community, as observed from field assessment activity and monitoring.
Monitoring Under the Project
Monitoring checklists were utilized under the project. The monitoring checklists were for a) 3As training at the Block level (2 days training) in 4 HPDs (pilot blocks); b) IPC at MCHN days in 4 HPDs (pilot blocks)and3As training at sector level (at sector meetings).
Monitoring Support for Mission Indradhanush(M.I.) and 3As
A nationwide campaign of M.I. was launched to address the problem of routine immunization of children left out or who dropped out. In Rajasthan, this campaign was organized in 13 high-priority districts. Under UNICEF SIHFW Partnership mentors and trainers had played the role of the monitor as well as a mentor at session sites of M.I.
The outcome of the above-mentioned ToTs has been achieved as per the objectives. The trained trainers/ resource persons have been rendering training sessions in block and sector level training in all 10 High Priority Districts. This includes training under SBCC partnership with UNICEF as well as training sanctioned by NRHM under PIP 2014-15. There was a convergence between NRHM (GoR) capacity building interventions and the SBCC Partnership. Rather than re-inventing the wheel by training a new set of trainers or repeating the ToT for NRHM IPC training, the same manpower trained in ToTs under SBCC partnership with UNICEF where the trainers in PIP training as well.
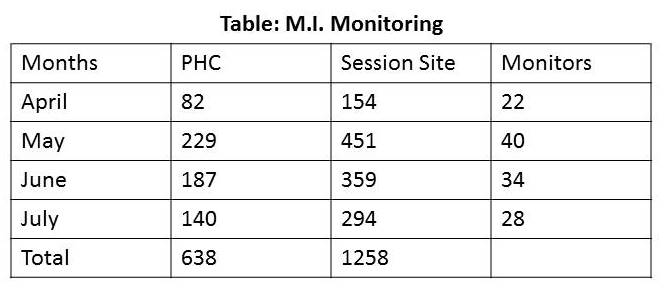
The table of M.I. monitoring indicates that in total more than 600 PHCs were monitored and more than 1200 session sites were monitored where Immunization was done under M.I., overall in all rounds of M.I.
To support the monitoring of M.I., IEC material for M.I. was also printed under the partnership. This included leaflets for community mobilization (for each date of each month (Round 1 to 4) to inform the community about M.I.The printed material was supplied to the districts and distributed to the community with the help of field functionaries. The branding concept of seven colors of the rainbow theme in M.I. was followed in the printed IEC material.
From the monitoring of M.I., it was observed that there was high visibility of IEC material printed under the partnership. Also, the presence of trained monitors helped the field functionaries in ensuring community mobilization. There were instances when most rigid communities also turned up for getting immunized after the involvement of trained monitors. The block-level planning process for organizing sessions under M.I. was also benefitted by the participation of monitors in block meetings and monitors helped in solving the problem at block and sector levels in a variety of works such as supply and demand generation.
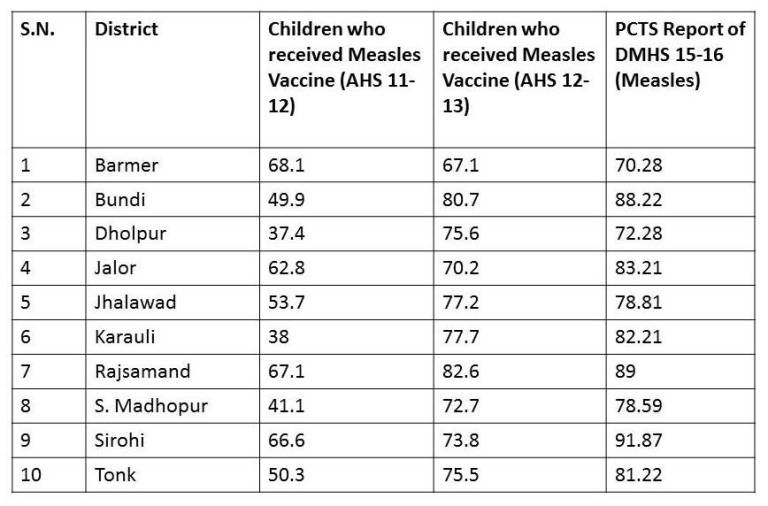
District-wise status of Immunization in HPDs indicates a continued to rise in Measles status over 2011-12, 2012-13, and 2015-16 years.
References:
- The Nursing Journal of India, Nov 2011
- Patient Education and Counseling, Vol 61, Issue 2, May 2006
- Social and Behaviour Change Communication (SBCC) Strategy for Routine Immunization in Rajasthan, 2014-15, State Institute of Health and Family Welfare (SIHFW, Rajasthan)
- Social and Behaviour Change Communication (SBCC) Strategy for RMNCH+A in Rajasthan, 2014-15, State Institute of Health and Family Welfare (SIHFW, Rajasthan)
- Bottleneck Analysis report by UNICEF, 2014
- URL:http://www.unicef.org/about/annualreport/files/India_Annual_Report_2014.pdf
- Rapid Assessment of Knowledge Attitude and Practice (KABP) on Continuum of Care by State Institute of Health and Family Welfare (SIHFW, Rajasthan), October 2009 (URL: http://www.sihfwrajasthan.com/studies/Report%20KABP.pdf
- Sample Registration System, Census 2013, (SRS) Bulletin, November 2014; Vol 49, No 1.
- Annual Health Survey (AHS)-Fact Sheet-Rajasthan, 2011-12 and 2012-13
- District Level Household & Facility Survey-RCH, No 3
* Associate Professor- Communication ** Director, *** Research Officer-Communication, at SIHFW
