Dr. V.R. Revathy*
Dr. I. Arul Aram**
Abstract
In HIV/AIDS communication, gender defines how programs respond to the needs of both men and women. Supportive environments should be created to have enough means of protection against the disease, besides care, when infected. This study on communication concerning HIV/AIDS is based on the following assumptions: (1) slum women are a higher risk population for HIV/AIDS and they need special attention; (2) television is the most effective media for propagation of HIV/AIDS messages; (3) public service announcements are widely used in HIV/AIDS communication. The research methods adopted for this study are discourse analysis of “Pulli Raja”, a televised PSA on HIV/AIDS, and focus group discussions among urban slum women in the 18-49 age group.
Introduction
Human Immunodeficiency Virus (HIV)/Acquired Immunodeficiency Syndrome (AIDS) is a great threat to humanity. HIV is a type of retrovirus that destroys the immune system of a human. Women in the lower socio-economic status are more exposed to HIV. HIV has spread across the world since the early 1980s to pandemic levels (Chavis 2012). Women are more likely to be exposed to HIV. Gender inequities in socio-economic status and patriarchal ideology around sexual practices are among the most important, yet often neglected, reasons for the feminization of this disease (Chong and Kvasny 2007). Gender inequities in abstinence, monogamy, and condom use are important factors in the feminization of HIV/AIDS that are often overlooked (Ojikutu and Stone 2005). The social ideology surrounding gender and power relationships is inevitably reflected and constructed in HIV/AIDS discourses (Cukier and Bauer 2004). The first AIDS patient in India was diagnosed by Dr. Suniti Solomon, a microbiology professor at the Madras Medical College, in Chennai in 1986.
In India, heterosexual mode of HIV transmission accounts for 88.2 percent of HIV positive cases detected, mother-to-child transmission accounts for 5 percent, infected syringe, and needle 1.7 percent, homosexual 1.5 percent, and contaminated blood and blood products account for 1 percent of HIV infections detected during 2011-12.
Need for study
Many HIV prevention programs have been carried out with a gender approach. Still, women do not have equal opportunities to benefit from the programs. Mendoza (1997) argues that these programs are related to gender roles in society and include sexual norms that limit women’s access to information by implying that they are ignorant about sexual matters. Women’s economic dependence on men, violence against women, and widespread acceptance of male promiscuity has worked against women’s chances of protection against the disease. Women are at greater risk of HIV infection from unprotected sex than men as they are often not in a position to negotiate with their partners because of the deeply entrenched patriarchy, particularly in Tamil Nadu. The major thrust of early programs was promoting ABC – abstinence, be faithful to partner, and condom use. Still CNN – which means condom use, safe needles, and negotiating with a partner – is yet to be adopted. In this context, the media can play a role in creating awareness and thus contributing to a change in behavior.
This study analyses the influence of the “Pulli Raja” Public Service Announcement (PSA) broadcast on television in creating HIV/AIDS awareness among women in slum areas, in Chennai, the capital of the Tamil Nadu province of India. PSA is one of the most effective means to create social awareness and bring about a behavior change. HIV/AIDS PSAs are intended to change the public interest, by raising awareness by informing people about HIV/AIDS, safer sex (condom usage), give up stigma and discrimination, and the importance of testing and counseling. Giving importance to family relationships and keeping off sex workers too are suggested but are not considered a must. PSAs, particularly on television, is expected to have direct or subtle influence among people and bring down the HIV/ prevalence.
Key populations with a higher risk for HIV include overcrowded low-income areas such as slums and slum clearance tenements. According to Goel and Dhaliwal (2004), a slum is an area of the city with inadequate housing, deficient basic requirements, overcrowding, and congestion. Socially, the slum is a way of life, a special character that has its own set of norms and values reflected in poor sanitation, health values, health practices, deviant behaviors, and social isolation. Thus, the slum problem is not only a problem of shelter; it is a problem of health and hygiene. Several widespread epidemic diseases emanate from the slums. These slums are not only a nuisance and danger to the slum dwellers but to the rest of the population.
Sex workers catering to the mobile population are normally either from the neighboring villages coming to the halt point during the day time or local tribe women, slum dwellers from the industrial towns located nearby, migrants or daily wage laborers from the construction sites, vegetable or fruit vendors at the halt points, etc. (NACO 2006). Hence, there is a need to study the influence of HIV/AIDS public service announcements used as part of major campaigns on television among slum women in Chennai.
Objectives of the study
To analyze the content of ‘Pulli Raja’ televised Public Service Announcement on HIV/AIDS in the Tamil language.
To ascertain the awareness level of slum women in Chennai towards transmission and prevention of HIV.
Defining keywords
Public Service Announcement (PSA) -is a public interest message disseminated by the media without any fee, to raise awareness, changing public attitudes, and behavior towards a social issue. It is a non-profit message distributed voluntarily through the media.
Slum -includes slums and slum clearance tenements in Chennai. These places are marked by small living spaces, crowded populations, unhygienic environment,s and lack of privacy.
Health Belief Model -is a model of behavior change that focuses on an individual weighing up the risks and benefits of behavior.
Self-efficacy – is an individual’s judgment of his or her ability to achieve a certain goal (such as not having unprotected sex).
Review of literature
The review of the literature revealed that innovative approaches have to be tried out to trigger behavioral change.
The use of mass media as a tool to promote HIV/AIDS awareness has been utilized extensively (Noar 2006). Although practitioners are now more realistic about the outcome of media use, it remains attractive to health practitioners due to its wide reach, appeal, and powerful nature alongside its cost-effectiveness (Randolf and Viswanath 2004).
Myhre and Flora (2000) confirm that the use of television in HIV and AIDS campaigns often resulted in higher message exposure in developed countries, whereas the developing countries have often used a mix of low-cost media such as radio and print materials.
According to Singhal and Rogers (2003), communication strategies represent a key ‘social vaccine’ against HIV. Communication is a necessary but not a sufficient, condition for preventing HIV/AIDS, and for augmenting care and support programs.
Dillard et al (1996) found that fear appeals such as those used in HIV/AIDS campaigns do much more than scare people; they evoke a variety of affective responses that have separate and unique effects on persuasion. To construct effective public health messages, campaign designers must begin to give explicit attention to the effective outcome of their persuasive appeals.
Approaches that effectively combine both behavioral and message design theories are more likely to be successful than those that use one without the other (Noar et al 2009).
Ackerson et al (2012) suggest that qualitative research methods such as focus groups and social mapping should be used to elucidate how similar messages can be differentially interpreted by people of different socio-economic positions. Television demonstrates the strongest association with higher knowledge and lower stigma.
Go et al (2003) in a study about HIV prevention messages and gender norms in slums of Chennai found that there is a direct linkage between marital violence and women’s ability to protect themselves from HIV/AIDS.
Theoretical framework
HIV/AIDS public service announcements come in various forms to cater to the needs of various audiences. This study tries to find out if the new trends in PSAs should replace older strategies, by examining the ‘Pulli Raja’ PSA text and its reception among the intended audience. The study uses the Health Belief Model.
The Health Belief Model (HBM) is a psychological model developed in the U.S. in the 1950s that explains and predicts health behaviors by focusing on the attitudes and beliefs of individuals. The key variables of the HBM are as follows (Rosenstock et al 1994).
Theoretical Proposition Of The Health Belief Model
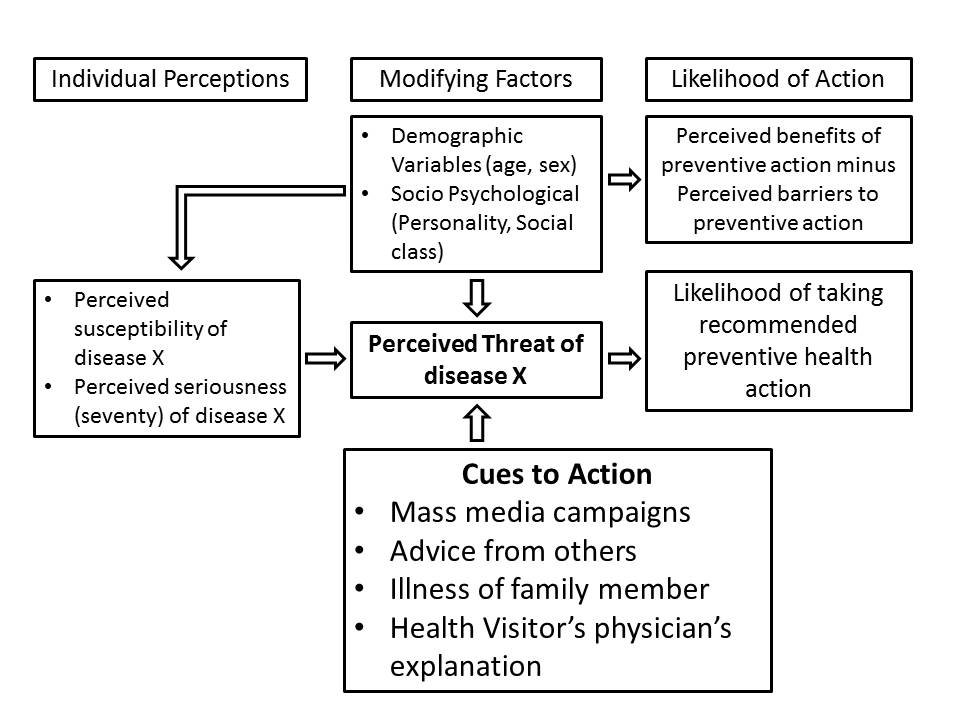 Figure 1 Health Belief Model
Figure 1 Health Belief Model
Methodology
This research went in for triangulation and used (1) Discourse Analysis and (2) Focus Group Discussion. Thus the research methods adopted for this study are discourse analysis of “Pulli Raja”- televised PSAon HIV/AIDS and the focus group discussions among urban slum women in the 18-49 age group.
In Discourse Analysis, interpretation arises from an act of reading or analysis which makes meaning of a text. Interpretations are based on contextualizing the text to social and historical realities. According to Fairclough (1995), interpretation focuses on three dimensions of discursive practice: (i) its manifestation in the linguistic form (in the form of ‘texts’); (ii) its instantiation of social practice (political, ideological and so on); and (iii) a third dimension which focuses on the socially constructed process of production, distribution and consumption which determine how texts are made, circulated and used. This study examined message factors such as theme, appeal, PSA characters, target audience, target message, female characterization, social reality, and gender.
Focus Group Discussion, or group interviews, served as a research tool for understanding audience attitudes and behavior. For this study, 10 to 15 people were interviewed simultaneously in different periods of time; with a moderator (woman counselor from a non-governmental organization who worked on HIV/AIDS) leading the respondents in a relatively unstructured discussion about HIV/AIDS awareness after the group viewed the PSAs.
Rogers and subsequent ‘diffusion’ studies concluded that the media was very important for increasing awareness but that inter-personal communication and personal sources were crucial in making decisions to adopt innovations (Waisbord 2012). Hence, slum and slum clearance tenements have been taken to make media intervention and to indulge in inter-personal communication which is much needed to translate awareness to action. The primary agenda for the Focus Group Discussions are to check the awareness level of HIV/AIDS among women and through which medium they get more information. Through this FGDs exercise, people were also able to move from awareness to action because of inter-personal communication.
The sampling technique is judgment sampling. Poor women in slums and slum clearance tenements in Kannigapuram, Kotturpuram, and Nochikuppam in Chennai city were chosen as samples, as slum people are assumed to be a high-risk group. The three slums are in different parts of Central Chennai. All three slums varied from one another in their characteristics. Slum areas were chosen for case studies using Focus Group Discussions as they are crime-prone, densely populated with many facilities shared, and promiscuity is high. Besides, the slums were accessible as non-governmental organizations were already working there.
In Kannigapuram, there are 38 streets. Similarly, in Kotturpuram, the tenements are 1,474 and it is situated adjacent to the Adyar river. The sample for study in Kannigapuramis from R and H blocks. 786 families are living in Nochikuppamalso known as Nochinagarsituated along the Bay of Bengal in and near the Light House area on Marina Beach. But the Nochikuppam slum clearance tenements are known for unhygienic atmosphere and, at least earlier, illegal activities such as sex work and illicit liquor. Demographic profiles of the samples include a detailed educational profile, economic profile, health profile, and media profile. The majority of the people that inhabit the slum tenements belong to the low-income category and are single-income families belonging to the labor class working in factories and industries and some as daily wage earners. Almost 40 percent of the sample includes illiterates and primary school dropouts while a little over 40 percent have crossed the secondary school stage of education. While three-fourths of the women are homemakers, some of them are adding to the family income by working as domestic help in well-off neighborhoods. The people living there predominantly belonged to the low-income category living in cramped one-room tenements which included space for living, sleeping, and a small extension for cooking. While some houses had separate bathrooms, others had shared toilet facilities. The streets were unclean with no facilities for garbage disposal. Most of the time, the streets were wet with random puddles of water not due to rain but because the folks had to fetch water from pumps at the street corner, or due to an unrepaired drainage system. Stagnant water served as a breeding ground for mosquitoes. Children played around in unhygienic environments while elders were seen cutting and cleaning fish right in the middle of the street with flies hovering around. People even rear cattle within the tenement. While these scenes reflect a typical day at the slum, it was encouraging to find that women cared a lot about the education of their children spending every extra pie on tuitions in the evening, a testimony to their aspirations of ensuring a stable and better future for the next generation.
Analysis and interpretation
For the purpose of this paper, one of the HIV/AIDS PSAs, ‘Pulli Raja’ has been analyzed in depth. ‘Pulli Raja’ is the most popular among the eight PSAs taken up for this study. The PSA had extensive reach as it was the first to shake the cultural taboo of not talking about sex in Tamil society. More so, it became popular as it was in the public arena for a longer period of time, and in multiple mediums including large hoardings.
Background:’Pulli’ usually refers to an important person. But it could be anybody who is as small as a dot (ordinary person in the society). ‘Pulli’ in the Tamil language is also a full stop or an end for something. The message is that anyone could be infected by HIV. ‘Pulli Raja’ is a representative of normal men, but also an important person with bad habits like consuming alcohol and visiting brothels. ‘Raja’, meaning King in the Tamil language and in other Indian languages as well, is also a common name in all strata of society. ‘Pulli Raja’ PSA started appearing in 2003.
To start with, ‘Pulli Raja’s’ identity was not revealed. The name itself suggests that he is a mischievous character. But such mischievous characters may look normal to the outside world. So first the question, “Will Pulli Raja get infected with AIDS [meaning HIV]?” followed by visuals of people from different walks of life under the same caption. Depicting people of different walks of life in the ‘Pulli Raja’ campaign implies that if you indulge in unsafe sex you will also contract HIV. Different people who repeat the same question in the PSA include common men from all walks of life. It serves as the reflection point for each man drawn from the different strata of society that everyone is susceptible to this deadly infection if he is not careful about his moral behavior, especially if he is a habitual drunkard and has unsafe sex with the sex workers. It is also implied that no individual should think that HIV infection would not affect him but only others. This ‘you’ appeal is to dispel the feeling even among the so-called respected people that they are immune to HIV infection.
Text of the PSA
Location: the local bar
Opening shot: Two men sitting across a table facing each other. They consume alcohol and are laughing.
A message is given by a man who drinks in the bar. He is portrayed as a participant, not as an observer or an outsider.
A waiter places water on their table.
Man 1:Will Pulli Raja get infected by AIDS?
Who is Pulli Raja? Is he a friend, an acquaintance?
Man 2:[Looks at him] If he is like you, he will get infected.
The person he is addressing is careless, easily gets drunk and visits brothels.
Man 1: [Moves to the edge of the seat in eagerness] Uh! How do you say?
He is nervous and tense; he is uninformed but concerned.
Man 2: If he gets totally drunk like you and goes after a woman, being too drunk to forget
wearing a condom even once, he might get infected by AIDS. [Fear appeal]
It implies that this character does it often. It also implies that persons like him will also have the same feeling.
Man 1:(A close-up shot of a shocked and guilty face)
Guilty face denotes that he himself has indulged in such activities.
Man 2: What?
Did you understand? [In a scolding and advising manner]
This is the manner adopted by film heroes too. In Tamil films, heroes are idolized. Their advice and their style of advice are taken seriously. The voiceover uses an interrogative. A voiceover is usually a voice of conscience. A third person is used for the voiceover. The viewers are asked to question themselves.
Voiceover: Does ‘Pulli Raja’ wear a condom each time?
The message is not to avoid wrong relationships completely but to be safer and protected in such relationships. The message is incomplete and makes the target audience to find an answer and decide.
Will Pulli Raja get infected by AIDS?
Analysis
In the ‘Pulli Raja’ PSA, viewers learned about the need for using condoms while going for sex with women.
Theme: Warning for drunkards, who would look for sex with sex workers!
Appeal: Emotional appeal of fear
PSA characters: Proximal characters
Target audience: Drunkards and sex workers
Target message: If you forget to use a condom when you are drunk and have sex with sex workers, you may get AIDS [HIV]. If your drunkard behavior has led you into unprotected sex with a sex worker, then there is every possibility that you may get AIDS [HIV].
Female characterization: No woman is visually portrayed in this PSA, but it warns the drunkards verbally that if you go after unknown women, you may get infected with HIV. The PSA is trying to reaffirm the Indian societal value system that it is always the woman about whom a man should exercise caution even though he himself is drunk and morally wrong. Here a stereotypical gender divide is constructed, which is pro-man. Discourse can be conventional and reproductive, accustoming people to accept it as common sense or fact; or creative and transformative, awakening people to realize alternative truths and make corresponding responses.
Social reality: The reason to portray a local wine shop could be that the men may not be conscious of their behavior when they are drunk, and to emphasize the probability that men meet each other there and socialize over a drink. It is like giving them a warning about their probable undesirable actions when they are drunk.
Gender: Sex workers are indirectly referred to as various women. Gender balance is like men are portrayed as drunkards and women as sex workers. According to Chong and Kvasny (2007), empowering HIV/AIDS prevention messages would, therefore, start from women’s daily-life experiences, lead women to question their original understandings about their own identities, and leverage the authoritativeness of the discourse providers to challenge ideologies that may heighten women’s risk for contracting HIV.
The following analysis is based on the Health Belief Model.
Perceived Susceptibility: In a conversation in ‘Pulli Raja’, the drunkard assumes his chances of getting infected and asks indirectly, will ‘Pulli Raja’ get infected by HIV?
Perceived Severity: The other person says that if he is like you, he will get infected by HIV. He moves to the edge of the seat (exhibiting the anxiety of probably getting infected with HIV) and asks “How do you say?” (Consequences).
Perceived Benefits: Even if they are not able to avoid having sex with sex workers, if they use condoms they can avoid getting infected by HIV.
Perceived Barriers: The close-up shot of shocking and guilty face shows the psychological barrier whether he will be able to stop the drinking habit, or will he be able to use a condom, if he is drunk and unconscious.
Cues to Action: After talking about the use of condoms the other person will ask in a screaming, advising manner, “Did you understand?” This is a reminder for others to follow.
Self-Efficacy: The final voiceover asks whether ‘Pulli Raja’always uses a condom. This builds confidence in one’s ability to use condoms to avoid getting infected by HIV.
Consequence: There was a sudden spurt in condom sales and use due to (at least partially) the high-recall of the ‘Pulli Raja’ campaign which screamed from billboards, bus panels, television screens, and cinema halls. The campaign had by then started moving into the villages as well.
The campaign, which was undertaken by the government in association with Population Services International (an NGO that addresses health problems of the low-income group and the populations lacking access to resources in developing countries), did come in for criticism from some quarters. In an attempt to stem risky behavior, it warned of the risks of having sex with sex workers if you are not protective and advised not to have sex with sex workers without using condoms. It promoted condom use rather than abstinence or being faithful to the partner. But then, it is not talking about morals when the society has gone a particular way and there is a need for action as a matter of emergency. They need to behave as a responsible human being or citizen is more compelling than being a morally good person. Sometimes, people who hold so-called high moral values slip from their moral standing by oversight. It can lead to disastrous consequences particularly in the context of sexual morality and HIV infection. This is because if self-righteousness is so high among people, they do not think of using condoms when they have pre-marital sex or extra-marital sex. Hence, direct condom promotion in PSA campaigns is much needed to break an adverse mindset against the use of condoms. ‘Pulli Raja’remains faceless throughout the campaign. He is every man, his conscience. He is an idea. This abstractness makes it easier for those in the target group to identify themselves with him. Showing the character’s face will lead people to develop associations and reject bad similarities with him.
An NGO worker was chosen as the facilitator for the FGDs for the reason that she was well-versed with the topic on hand and had vast experience in dealing with slum women. Women participants from the slums were not identified by names because HIV/AIDS discourse is still a taboo among women in Tamil Nadu. The women participants too made a specific request not to be identified by name and they even suggested that their slum clusters be not identified if possible.
In the 39-49 age group, many women were able to say that HIV spreads through an illegal sexual relationship, use of dirty injection needles, and blood transfusion. Mass media messages about HIV/AIDS prevention have been associated with correct conceptions about the modes of HIV transmission. The 30-38 age group is much feared about HIV/AIDS and the women in the group say HIV spreads mainly because of their husband’s drinking habit, and the men are suspected of having sex with sex workers as well.
Many believe that HIV/AIDS can be cured and when the moderator questioned them further they said that they came to know it through the media which always says that HIV/AIDS people can lead a normal life. This means that the women misunderstand that leading a normal life by retroviral treatment through drugs as ‘cure’. A similar finding by Kalasagar et al (2006) among Chennai slum dwellers also says that 71 percent of females feel that AIDS can be treated with either costly medicines or at least by traditional herbal medicine.
Most of the women said that they never discuss HIV/AIDS with their husbands. One participant shared her experience that when she started asking about HIV/AIDS, her husband scolded her saying that it is very dangerous, and told her not to talk about it. Then many women followed up with their remarks saying that it is very tricky to discuss HIV/AIDS with their husbands. The reason why they do not want to discuss this with their husbands is that either they will be in trouble, putting them in an embarrassing situation or their husbands may think that their husbands might have extra-marital relationships or sex with sex workers. However, a few women agreed that they try to avoid having sexual intercourse when the husbands are drunk. Many women agreed that they were not able to handle such situations. Participants felt that they need to have the right persons to discuss this issue and they always wait for someone to initiate this topic. It is taboo to talk about sexual matters in the community and if they do so, they will get a bad image in the community. But they started interacting with the counselor-moderator who conducted the focus group discussions though she is new to them and they become even more comfortable after watching the PSA. So frequent exposure to media messages will definitely improve inter-personal communication and help them to overcome the taboo, as open discussion is necessary to make informed, right choices.
In fact, a sex worker from one of these slums who took part in a focus group discussion said, “Sex workers insist that their customers use condoms”.To achieve his, the sex workers either convince or force the men. They also keep a stock of condoms. But many ‘family’ women do not have this power, which they too must have given the fact that many a husband has sex elsewhere too. According to the sex workers, because of this lack of negotiating power among most ‘family’ women, the HIV prevalence rate is bound to increase among women with their husbands as a single partner, though the rate is bound to decrease among sex workers. A good number of slum tenement women are Dalits. Unlike caste Hindus, Dalits do not practice patriarchy to a large extent. But then, callousness is widely prevalent among low-income women, and added with it is the problem of alcoholism prevalent among most Dalit men, if not women. People of Kotturpuram slum tenements are mostly Dalits, whereas those of the other two areas under study constitute people of various backward castes besides Dalits.
Newmann et al (2000) study rightly concluded: HIV prevention and intervention strategies need to focus on married, monogamous Indian women whose self-perception of HIV risk may be low, but whose risk is inextricably linked to the behavior of their husbands.
Core cultural values also act as barriers because many said that people who are religious and have faith in God will not get any such disease and they need not listen to this kind of information. But then faith may fail them because of human frailty and if a person indulges in unsafe sex outside marriage, he may be infected with HIV.
Campaigns that take the wider environment into consideration are more likely to be achieved and sustainable in the long term. In fact, peer education is a major factor that can turn knowledge passed on by mass media into behavioral change. Myhre and Flora (2000) consider that mass media campaigns should also aim to include communities, rather than just focussing on individuals. In HIV campaigns they propose that mass media should increase the importance of prevention, frame HIV as a community issue, improve ‘discourse’ around HIV, and improve the nature of participation in HIV. An effective mass media campaign for HIV, therefore, would have to collaborate with interventions that are aimed at improving the structural, economic, or environmental conditions of a community or communities.
Many women were reluctant to speak about condom use and many do not have any idea that condoms can prevent HIV infections, except a few who have their relatives working as nurses or outreach workers. But gone are the times when people did not know how to use the condom and had sex after swallowing a condom thinking that it was a medicine, or had sex wearing a condom in a thump finger because a social worker had demonstrated to them the condom use that way!
Though ‘Pulli Raja’ focussed on the use of condoms, the message has not reached the female slum community. Many misinterpret that AIDS can be cured and only weak people are affected by HIV/AIDS. The environment in the widest sense could include aspects such as schooling or education. Mbananga and Becker (2002) suggest that poor cognitive skills can result in non-understanding of the messages, and the importance of formal education as a foundation for individuals and groups. This suggests that the addition of education into the wider environmental and societal area may be important in interpreting health promotion messages through the media.
There is no clear idea about preventing parent-to-child transmission (PPTCT) but all married women knew that they do HIV tests during pregnancy. Only one participant whose daughter is working as a nurse can tell that if the HIV-positive pregnant women take proper treatment, there are chances of delivering an HIV-negative baby. Many women said that all kinds of treatment related to HIV are available in government hospitals.
In Kannigapuram, one participant said a woman died of HIV/AIDS, but her husband and children who are also HIV-positive are still alive. The blame was put on the woman as if it is she who transmitted the virus to the husband and children. That was the reason she died before them. The truth is that she was married to an HIV-positive man without knowing it. Her in-laws, despite knowing that he was HIV-positive, arranged for the marriage to make their son happy and also to beget grandchildren through him. The participant said that it is advisable that before finalizing the life partner, every other factor and health status be considered carefully by both the families.
In a focus group discussion in Nochikuppam, one outreach worker narrated a real-life incidence of a student living with HIV who was treated badly in the school by some students and teachers. Hence the HIV-positive student discontinued the studies and stopped taking medicines too, which badly affected her health. The narration of this story received a response from other participants who said that they can face any kind of hurdles in life but they should not put their children into trouble.
One participant in a focus group discussion talked about her drunkard husband’s behavior, which often threatens her exposure to HIV. This made other women in the group pursue the line of argument and many said that despite opposition from their husbands to an HIV test during pregnancy they manage to get it done. As the researcher used an HIV/AIDS counselor as the moderator, the discussion had a beneficial snowballing effect and many respondents commented on the views of others.
Findings
The study found that women of urban slums and slum clearance tenements are poor and they lack awareness of HIV/AIDS. More so, their environment is not conducive to taking enough precautions against HIV. Although the inhibition of talking about sex is not much among this class particularly because of minimal patriarchy prevalent at the lower end of the social spectrum, awareness about HIV/AIDS is definitely lacking and callousness about the spread of HIV/AIDS is widespread. The study agrees with much of the findings of Gautam et al (2008) study on awareness, knowledge, and misconceptions about STIs and HIV/AIDS in India. Discussing sensitive issues around sexuality, critical to effective AIDS education, requires a change of traditional ‘culture of silence’ so people can more freely talk about sex. Comprehensive awareness, leading to attitudinal and behavioral change in individuals and society towards safe sexual and other health practices, is the only weapon today against HIV/AIDS. HIV/AIDS among women is an important health problem in India. There is evidence that limited knowledge and misconceptions about HIV/AIDS would lead to higher-risk sexual behavior. The marital relationship can be an environment of risk in which there are major barriers to safer marital sex, poor marital communication about sexual risk and sexuality, limited capacity for a wife to husband demand for sex, and limited use of condoms in marital sex as protection against disease transmission. A significant number of Indian women lack control over their sexual lives and this is made more severe by domestic violence, coercive sex, and cultural constructions of gender that contribute to HIV/AIDS risk among married women. These factors of risk within marriages are amplified by poverty, illiteracy and gender discrimination, arranged marriages to virtual strangers, poor marital relationships, and limited social support.
The Health Belief Model begins with ascertaining the knowledge, attitudes, behavioral interventions, and behavioral practices of individuals regarding HIV prevention, care, and support. Gaps in knowledge, attitudes, and behaviors among the target audience were identified through focus group discussions so that deficiencies in communication interventions for a higher risk group like slum women could be addressed in the future.
The urban slum and slum clearance tenements women -with diverse influences – often rejected or dissociated themselves from the messages and the media through which they were communicated. The strongest identification with the messages and participate in the campaigns were observed among the women who spent much time in other informative programs, who discuss those with the spouse and other fellow women, or who are involved in social activism like self-help groups or community radio programming. The inter-personal discussions happened in women self-help groups, capacity-building programs organized by non-governmental organizations, or at times of other social activism as well. To retain the knowledge gained, there is a need for direct, hard-hitting messages, particularly for slum people. PSA characters make the viewers identify with the characters and if the identification is stronger and messages clear enough, intended communication happens.
Women in slums are doubly discriminated against – they are ‘the other of the other’. They are neglected and disempowered first since they are slum-dwellers, and second because they are women. Women who are victims of sexual violence are at a higher risk of being exposed to HIV. The lack of condom use means that women are immediately more likely to be exposed to HIV infection. Abused wives face increased HIV risk based both on the greater likelihood of HIV infection among abusive husbands and elevated HIV transmission within abusive relationships.
Focus group discussions revealed that ‘fear appeal’ many a time does not evolve as a positive change in behavior, so it cannot be considered the right approach. This is probably true of slums that have diverse harsh influences, unlike the rest. This finding, however, contradicts that of Dillard et al (1996) that fear appeals such as those used in HIV/AIDS campaigns do much more than scare people; they evoke a variety of affective responses that have separate and unique effects on persuasion.
Women in slums lack education. Education for lower socio-economic status girls should be improved. They should be empowered particularly by giving information on HIV/AIDS-related preventive measures in a printed format and distributed in forms such as notices, which they can use whenever they have any doubts, and they can even share it with others and gain in terms of peer education. This eagerness to learn in a structured way is more present among the young women in the 18-28 age group. All women need to have health programs in their community with interactive sessions to clarify their doubts with an HIV/AIDS counselor.
References
- Ackerson, Leland K, Ramanathan, Shoba, Arya, Monisha, and Viswanath, Kasisomayajula, “Social Disparities, Communication Inequalities, and HIV/AIDS-Related Knowledge and Attitudes in India”, AIDS and Behaviour, Volume 16, Issue 7, pp.2072-2081, October 2012.
- Chavis, Jason. “About HIV”, eHow: Health Topics A to Z,
http://www.ehow.com/about_4691097_hiv.html?ref=Track2&utm_source=ask Accessed on 30 November 2012. - Chong, Jing, and Kvasny, Lynette. “A Disease That ‘Has a Woman’s Face’: The Social Construction of Gender and Sexuality in HIV/AIDS Discourses”, Intercultural Communication Studies XVI: 3, 2007. 1-13. Accessed from
http://www.uri.edu/iaics/content/2007v16n3/04%20Jing%20Chong%20&%20Lynette%20Kvasny.pdf - Cukier, W. and Bauer, R. “Applying Habermas’ validity claims as a standard for critical discourse analysis”, in Information Systems Research: Relevant Theory and Informed Practice, B. Kaplan, D. Truex III, D. Wastell, T. Wood-Harper, and J.I. DeGross. Eds. Kluwer Academic Publishers, Boston, 2004.
- Dillard, James Price, Plotnick, Courtney A., Godbold, Linda C., Freimuth, Vicki S., and Edgar, Timothy. “The multiple Affective outcomes of AIDS PSAs: Fear Appeals do more than scare people”, Communication Research, Sage Publications, Volume 23; pp.44-72, February 1996.
- Fairclough, Norman. Critical Discourse Analysis: The Critical Study of Language, Pearson Education Limited, Harlow, 1995.
- Go, V.F., Sethulakshmi, C.J., Bentley, M.E., Sivaram, S., Srikrishnan, A.K., Solomon S., and Celentano, D.D. “When HIV-prevention messages and gender norms clash: the impact of domestic violence on women’s HIV risk in slums of Chennai, India”, AIDS Behav 7(3): pp.263-72, 2003.
- Goel, S.L. and Dhaliwal, S.S. Slum Improvement through Participatory Urban-Based Community Structures, Deep and Deep Publications, New Delhi, 2004.
- Mbananga, N. and Becker, P. “Use of technology in reproductive health information designed for communities in South Africa”, Health Education Research, 17(2), pp. 195-209, 2002.
- Mendelsohn, H. “Which shall it be: mass education or mass persuasion for health?” American Journal of Public Health, 58, pp.131-137. 1968.
- Mendoza, R. Quoted in Encyclopedia of AIDS, G.C. Satpathy, Ed. Kalpa Publications, New Delhi, 1997.
- Myhre, S.L. and Flora, J.A. “HIV/AIDS communication campaigns: Progress and prospects”, Journal of Health Communication (Supplement1), 5, pp.29-45, 2000.
- Myrick, Roger. “Making women visible through health communication: representations of gender in AIDS PSAs”, Women’s studies in Communication, Volume 22, Issue 1, pp.45-65, 1999.
- NACO. “Strategy and Implementation Plan of NACP-III”, National AIDS Control Organization, Ministry of Health and Family Welfare, Government of India, 2006.
- Newmann, S., Sarin, P., Kumarasamy, N., Amalraj, E., Rogers, M., Madhivanan, P., Flanigan, T., Cu-Uvin, S., McGarvey, S., Mayer, K. and Solomon, S. “Marriage, monogamy and HIV: a profile of HIV-infected women in south India”, International Journal of STD & AIDS, Vol. 11, No.4, pp.250-253, 1 April 2000.NFHS-3 (India: National Family Health Survey 2005-06). IIPS, Mumbai, 2007.
- Noar, Seth M., Palmgreen, Philip, Chabot, Melisa, Dobransky, Nicole and Zimmerman, Rick S. “A 10-year systematic review of HIV/AIDS mass communication campaigns: have we made progress?”, Journal of Health Communication, Volume 14, pp.15-42, 2009.
- Ojikutu, B.O. and Stone, V.E. “Women, inequality, and the burden of HIV”, The New England Journal of Medicine, 352(7), pp.649-652. 2005.
- Rosenstock, I.M., Strecher, V.J., & Becker, M.H. “The health belief model and HIV risk behavior change”, in R.J. DiClemente and J.L. Peterson in Preventing AIDS: Theories and Methods of Behavioural Intentions, Eds. Plenum Press: New York, pp.5-24, 1994.
- Singhal, Arvind, and Rogers, Everett M. Combating AIDS: Communication Strategies in Action, Sage Publications, New Delhi, 2003.
- Waisbord, Silvio. “Family tree of theories, methodologies, and strategies in development communication”, The Rockefeller Foundation, Accessed on 30 November 2012. http://www.communicationforsocialchange.org/pdf/familytree.pdf
* Assistant Professor, Department of Media Sciences
** Associate Professor, Department of Chemistry,
Anna University, Chennai, India.
